









 6 / 14
6 / 14

6
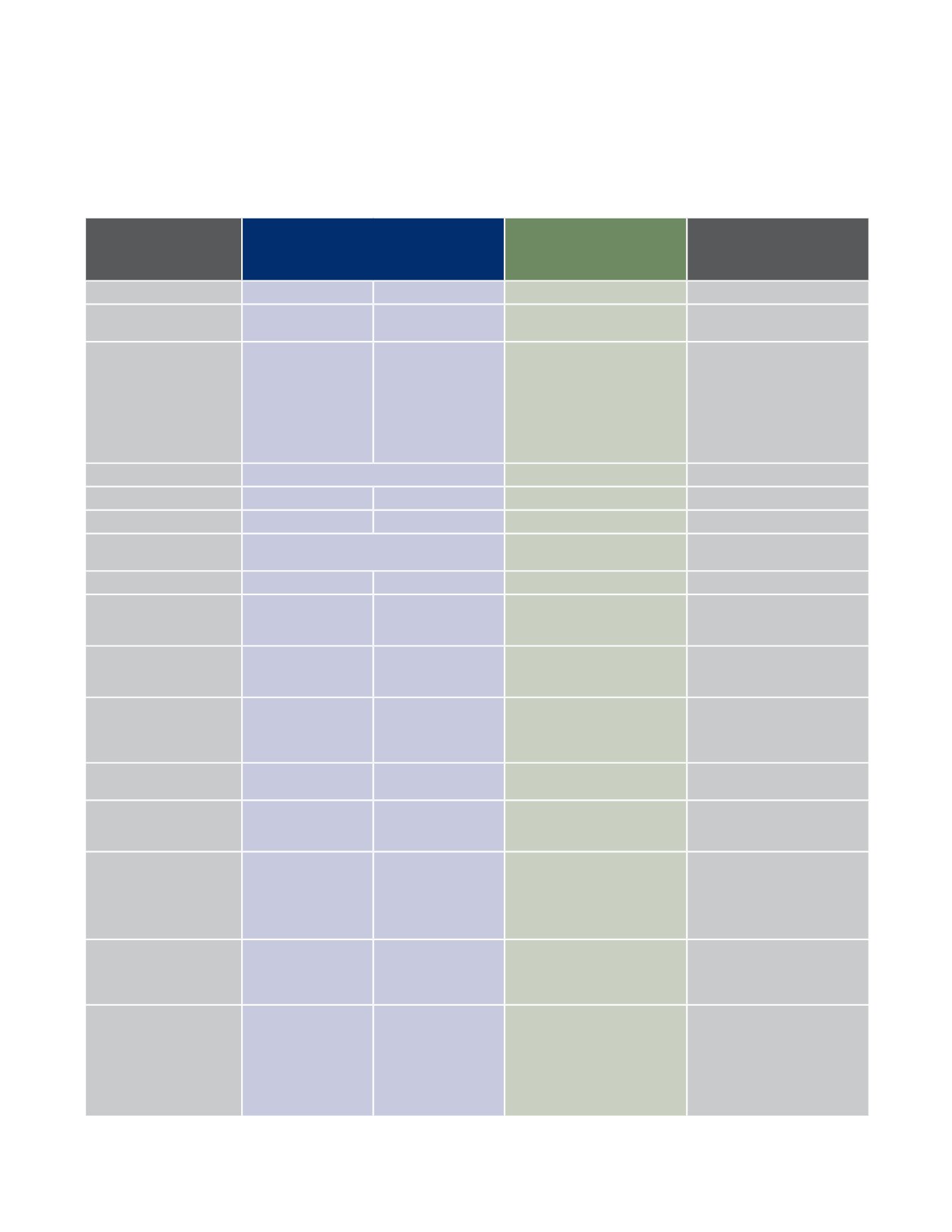
LAPRA Medical Plans At-a-Glance
The table below provides an overview of the key benefits provided through the LAPRA medical plans. Please refer
to the Anthem Blue Cross PPO or HMO, or Kaiser HMO materials for a complete description of benefits including
terms of coverage, exclusions and limitations.
Benefit Feature
Anthem Blue Cross
Prudent Buyer PPO
Anthem Blue Cross
CaliforniaCare Plus HMO
(California Residents Only)
Kaiser
HMO
(California Residents Only)
Providers
PPO Network Non-PPO Network
1
HMO Providers Only
3
HMO Providers Only
Calendar Year
Deductible
$300 per person
$600 per family
$500 per person
$1,000 per family
N/A
N/A
Calendar Year Out-of-
Pocket Maximum
(includes deductibles and
co-pays; excludes co-pays
for infertility benefits)
Medical Charges:
$2,000 per person
$6,000 per family (not
to exceed $2,000 for
any one person) See
page 7 for prescription
drug out-of-pocket
maximum.
Medical Charges:
$3,000 per person
$9,000 per family (not
to exceed $3,000 for
any one person) See
page 7 for prescription
drug out-of-pocket
maximum.
Medical and
Prescription Drug Charges:
$1,000 per person
$3,000 per family
Medical and
Prescription Drug Charges:
$1,500 per person
$3,000 per family
Lifetime Max
Unlimited
Unlimited
Unlimited
Office Visit
90%
2
70%
2
$15 co-pay
$15 co-pay
Hospitalization
90%
2
70%
2,4,5
100%
100%
Emergency Room
90%
2
after a $150 co-pay
(waived if admitted)
$150 co-pay
(waived if admitted)
$150 co-pay
(waived if admitted)
Urgent Care
90%
2
70%
2
$15 co-pay
$15 co-pay
Maternity Care
90%
2
70%
2
Doctor visits: $15 co-pay
(initial visit only)
Facility charges: 100%
Doctor visits: 100%
Facility charges: 100%
Well Baby/ Child Care
100%
(up to age 7; not
subject to deductible)
70%
2
(up to age 7; not
subject to deductible)
100%
(up to age 7)
100%
(up to age 2)
Routine Physical
100%
(adults & children over
age 7; not subject
to deductible)
Not covered
100%
(adults & children over age 7)
100%
Diagnostic X-ray
& Lab Tests
90%
2
70%
2
100%
100%
Body Scans
(not subject to
deductible)
100% after $25
co-pay; up to $250
per calendar yr
Not Covered
Not Covered
Not Covered
Physical & Occupational
Therapy and
Chiropractic Services
(additional services may be
authorized)
90%
2
(24 visits per calendar yr
combined PPO Network
& Non-PPO Network)
70%
2
(24 visits per calendar yr
combined PPO Network
& Non-PPO Network)
$15 co-pay
(limited to a 60-day period of
care after illness or injury;
additional visits available when
approved by the medical group)
$15 co-pay
(Chiropractic up to 40 visits per year)
Acupuncture
90%
2
(24 visits per calendar yr
combined PPO Network
& Non-PPO Network)
70%
2
(24 visits per calendar yr
combined PPO Network
& Non-PPO Network)
$15 co-pay
$15 co-pay
Mental Health/
Chemical Dependency
• Outpatient
• Inpatient
90%
2
90%
2
70%
2
70%
2,4,5
$15 co-pay
100%
$15 co-pay individual therapy/
group therapy: $7 co-pay
mental health,
$5 co-pay chem dep
100%
1
Benefits are based on the customary and reasonable charge. You are responsible for any difference between the amount charged and the
customary and reasonable charge, plus any deductible and/or coinsurance amount.
2
Subject to calendar year deductible.
3
Your primary care physician can refer you to a specialist when necessary and must approve all care you receive except in the event of an emergency.
4
Failure to obtain pre-service authorization may result in a $350 penalty.
5
Covered expense is reduced by 25% for services and supplies provided by a non-contracting hospital.